
Sammanfatta detta blogginlägg med:
Editor’s note: This article is part of Polestar Analytics’ commercial-excellence series for life sciences. Impact ranges reflect outcomes observed across Polestar Analytics engagements and the firm’s published analysis; third-party figures (Deloitte, McKinsey) link to their original sources. Further reading: our take on why AI in pharma stalls
TL; DR — Traditional HCP segmentation is rebuilt once a year on prescription volume alone, so the target list is stale for much of its life. For teams evaluating hcp segmentation in pharma industry, this provides a practical roadmap from static lists to living intelligence. Agentic AI turns it into a continuous, self-service system that unifies data, scores every HCP, predicts behaviour, and recommends the next best action & learns from the result. HCP segmentation in Pharma is no longer just about ranking physicians by volume; it is about understanding who to engage, when to engage, and through which channel. This guide explains what modern HCP segmentation is, why legacy models fail, the five-step framework that replaces them, and the business impact teams report.
- Treat segmentation as a living system, not an annual deck — the market moves between refreshes, and so should your targeting.
- Volume alone is a weak signal. Loyalty, channel sensitivity, switching risk, and clinical potential explain why an HCP prescribes and how to engage them.
- The closed loop is the differentiator — recommendations that learn from outcomes beat static lists every cycle.
- Impact is measurable: priority-segment Rx, promotional efficiency, field productivity, and decision speed all move when effort follows evidence.
Most pharma commercial teams are sitting on more HCP data than they’ve ever had, and using a fraction of it. Prescribing feeds, claims, CRM notes, email opens, payer files. With all pouring in, while the HCP segmentation that decides where reps spend their week is still rebuilt once a year and ranked mostly on prescription volume. This is why hcp segmentation for pharmaceutical companies needs to become more dynamic, data-led, and connected to daily field decisions.
That gap is expensive. In Deloitte’s 2026 Life Sciences Outlook, 32% of biopharma executives flagged customer engagement as a significant concern, and nearly half named accelerated digital transformation as a defining trend for the year. The problem was never collecting data rather acting on it before the moment passes.
Traditional HCP segmentation in Pharma fails because they’re built once a year on prescription volume alone, while HCP behaviour, channels, brand dynamics, and payer mix change continuously. So, the list is outdated for much of its life, and reps act on stale priorities. This is why hcp segmentation in pharma industry needs to move beyond annual deciles and into continuously updated decision systems.
Ask a few honest questions about your current segmentation setup and the cracks show. Most legacy HCP segmentation frameworks share the same limits:
- Static and manual. Built on fixed rules and heavy manual effort, so insights arrive late.
- Data left on the table. Nearly half of available data goes unused in traditional models.
- Leaders feel it. Around 95% of leaders worry that slow, data-poor decisions are hurting performance.
- Volume-only, refreshed yearly. Ranked mostly on TRx and specialty, yet a meaningful share of HCPs shift segments within six months. Hence an annual list is stale for much of the year.
- Lagging, partial data. Claims land 15 to 45 days after the script, and many programs fund just 20 to 25 data sources when closer to 40 give the full picture.
These HCP segmentation challenges surface as missed prescribers, wasted promotion, and reps calling on physicians who were never going to switch. Industry estimates put the annual toll of fragmented data and delayed insights above $150 billion. And it’s rarely a tooling shortage: across industries, McKinsey’s latest State of AI survey found 88% of organizations now use AI somewhere, yet only about 6% capture real value from it. The constraint is operationalizing it.
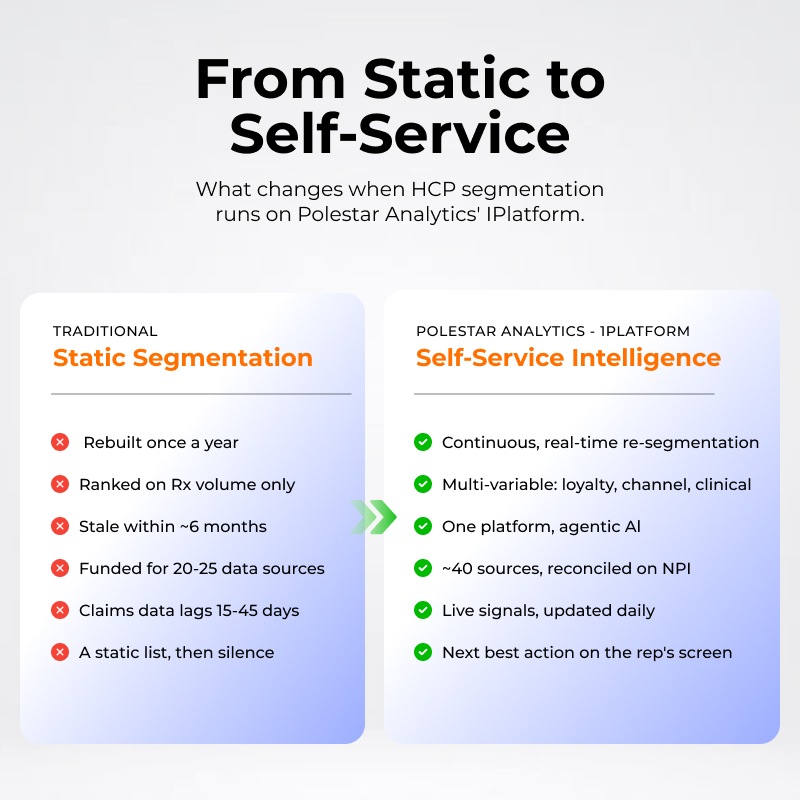 From static, annual, volume-only lists to real-time, multi-variable intelligence.
From static, annual, volume-only lists to real-time, multi-variable intelligence.
In short: Agentic AI employs segmentation that continuously functions in a loop. The agent can sense a new or changing signal, determine whether or not the signal is new or has changed, make an actionable recommendation based on the analysis and then learn from the outcome. Compared to traditional segmentation which only refreshes annually and can take time (usually weeks) before a recommendation can be acted upon.
The shift sounds simple but quite difficult to engineer. Static to self-service. Rather than a quarterly project that data science hands down to the field, HCP segmentation in pharma becomes a living system. Traditional models segment once and react in weeks; agentic AI senses, decides, acts, and learns daily, which matters because channel behaviour, brand dynamics, and patient mix change daily too.
In practice, that system needs to live in one place. On Polestar Analytics’ 1Platform, data, models, and recommendations sit in a single governed environment, and agentic AI pushes the next best action straight to a rep’s screen rather than into a dashboard nobody opens. We call the layer that runs continuously across this environment the Agentic Brain — and the two-minute walkthrough below shows what it looks like when a sales rep opens 1Platform in the morning.
The teams that win the next launch cycle won’t be the ones with the most data — they’ll be the ones who turn it into a daily decision. Segmentation has to become an operating system, not an annual deck.
A durable framework runs as five connected steps, each driven by a purpose-built AI agent rather than a stack of disconnected tools.
- Intelligent data foundation — a DataSync agent unifies every Rx, claim, CRM, and digital signal into one NPI-keyed HCP view.
- Dynamic AI segmentation — clusters that evolve with real-world behavior, not once a year.
- Scores that explain prescribing — loyalty, channel sensitivity, promotional response, therapeutic competitiveness, clinical potential, and switching-risk, quantified for every HCP.
- Predictive targeting — forecasts Rx growth, churn, and switch risk, then ranks HCPs by expected return.
- Closed-loop next best action — recommends the right message, channel, and timing, then learns from every outcome to sharpen the next.
 Polestar Analytics’ five-step, closed-loop engine — one purpose-built AI agent per step.
Polestar Analytics’ five-step, closed-loop engine — one purpose-built AI agent per step.
The final loop is what separates a report from a system: every action feeds the next decision, so the model gets sharper the more the field uses it. For the wider playbook, this ebook on agentic AI types, use cases, and workflows walks through how these agents fit together.
In short: Teams that move to dynamic, AI-driven segmentation report meaningfully higher prescriptions in priority segments, less wasted promotion, faster decisions, and more converted non-writers — because effort follows evidence instead of last year’s deciles. For commercial teams, hcp segmentation for pharmaceutical companies becomes most valuable when it directly improves targeting, engagement, and prescription outcomes.
When a commercial team makes this shift, the gains compound across the funnel:
- 20–40% more Rx among responsive physicians when targeting follows loyalty and channel-sensitivity scores.
- Up to 4x uplift in Rx productivity, with a multiple-fold lift in effective reach.
- 20–30% less promotional waste.
- 30–40% gains in field-force productivity — reps know who, how, and when to engage each day.
- 70–80% faster decision cycles.
- Up to 50% of high-potential non-writers converted.
What would spotting a rising prescriber 60 days early, or pulling a third of your spend off the wrong targets, be worth this year?
Plenty of vendors sell a slice of this. Polestar Analytics delivers the whole engine on one platform. The agentic AI, life-sciences domain depth, and last-mile delivery: real-time instead of periodic, multi-variable instead of volume-only, enterprise-grade for top-20 and emerging brands alike. For organizations modernizing hcp segmentation in pharma industry, Polestar Analytics brings the data foundation, AI agents, and execution layer together.
Decile and ABC models rank HCPs almost entirely on past volume and refresh on a fixed calendar. Dynamic segmentation adds behavioural, channel, and predictive signals and updates continuously, so a fast-rising prescriber doesn’t sit in a low tier for a year before anyone acts on it.
Many programs run on 20 to 25 because that’s what budgets allow, but a complete picture usually needs closer to 40 — Rx, claims, CRM, digital, payer, and KOL signals among them. The point isn’t volume for its own sake; gaps in source coverage are where targeting errors come from.
Traditional segmentation is usually refreshed just once or twice a year, yet a meaningful share of HCPs shift segments within about six months. Running ingestion, clustering, and scoring continuously on one platform closes that lag to near real-time — and emerging or specialty teams can stand it up faster than a full custom build.
It’s a 0–100 measure of how responsive a physician is to each channel — email, e-detailing, webinars, field calls, MSL visits. Scoring it per HCP tells you not just whether to engage someone but where, so a digital-first prescriber isn’t getting in-person visits they’ll never accept while budget is pulled from someone who would.
No, it sharpens it. The agents handle the analysis (who to see, on what, and when) so reps spend their time on the conversations that move prescriptions, with the next best action delivered in their existing workflow rather than a separate dashboard.